Do Antioxidants Actually Improve Fertility? What a 2024 Meta-Analysis of 20 Trials Found
Publication 16
Antioxidants and Fertility: What 20 Trials Found
If you've been told your ovarian reserve is low or your eggs are "aging," you've probably been handed a supplement protocol — CoQ10, melatonin, maybe a handful of others — without much explanation of why, at what dose, or whether the evidence actually supports it.
The research does exist. It's just rarely presented in a way that lets you evaluate it.
A 2024 systematic review and meta-analysis published in Advances in Nutrition is the most comprehensive analysis to date on this question. It pooled data from 20 randomized controlled trials involving 2,617 women specifically with ovarian aging — not general infertility — to find out whether antioxidant supplements actually move the needle on reproductive outcomes.
The answer is more nuanced than most supplement advocates or skeptics will tell you.
Why This Meta-Analysis Is Different From Most Fertility Supplement Research
Study type: Systematic review and meta-analysis of 20 randomized clinical trials (RCTs)
Published:Advances in Nutrition, 2024 (Shang et al.)
Participants: 2,617 women with ovarian aging, categorized as advanced age (over 35), diminished ovarian reserve (DOR), or premature ovarian insufficiency (POI)
Goal: To evaluate whether antioxidants improve reproductive outcomes during IVF, and to identify optimal dosing protocols
Why a meta-analysis matters here: pooling data across 20 trials reduces the risk that one small or biased study skews the result. It is the highest-level evidence available short of a single massive trial, and for this population, no single massive trial exists.
The antioxidants studied included CoQ10 (at doses ranging from 30 mg/day to 1200 mg/day), melatonin (2–16 mg/day), myo-inositol (4 g/day), vitamin D3, vitamin E, resveratrol, and a combined antioxidant preparation. Treatment durations ranged from a single administration to three months before ovarian stimulation.
The primary outcomes the researchers cared about most: live birth rate and clinical pregnancy rate. Secondary outcomes included egg quantity and quality, embryo quality, gonadotropin dose required, miscarriage rate, and adverse events.
What the Data Found:
Pregnancy Rates, Egg Quality, and the Live Birth Gap
The gap between clinical pregnancy and live birth
This is the most important distinction in the entire paper, and it gets lost in most summaries.
Antioxidants significantly increased clinical pregnancy rates — meaning confirmed intrauterine pregnancies — by a meaningful margin. The odds ratio was 1.55 (95% CI: 1.18–2.04, p=0.002), based on 21 trials involving 2,218 women. That's a statistically robust finding with moderate evidence quality.
Live birth rate is a different story. Seven trials with 1,224 participants measured whether antioxidants resulted in more actual babies born. The odds ratio was 1.05 (95% CI: 0.80–1.37, p=0.74). That confidence interval crosses 1.0 — the "line of no effect" — meaning the data does not prove that antioxidants increase live births. The evidence quality for this outcome is rated low.
This doesn't mean antioxidants don't help. It means the studies that measured the outcome that matters most to patients were too few and too small to reach a definitive conclusion either way.
Egg quantity, embryo quality, and ovarian sensitivity
More eggs retrieved. Women taking antioxidants had slightly more eggs collected during their retrieval — just under one extra egg on average. That sounds small, but it was consistent across 15 trials, which makes it a reliable signal rather than a one-off result. (MD: 0.98; moderate evidence)
Better embryo quality. The proportion of good-quality embryos was more than double in the antioxidant group compared to women who took no supplement. This is one of the more striking numbers in the paper, though it comes from only three trials, so it needs to be confirmed in larger studies before anyone should treat it as settled. (OR: 2.32; low evidence)
Mature egg count did not clearly improve. Researchers also looked at whether antioxidants increased the number of mature eggs specifically — the ones actually capable of being fertilised. Here the results were all over the place. Some trials showed a benefit, others did not, and the inconsistency was too high to draw a meaningful conclusion. (Very low evidence — treat this outcome as unknown for now)
The ovaries needed less medication to respond. During IVF stimulation, women take hormone injections to encourage the ovaries to produce eggs. Women taking antioxidants needed significantly less of this medication — roughly 243 fewer units on average — meaning their ovaries were more responsive to lower doses. For women who have previously been poor responders to stimulation, this is a clinically meaningful finding. (MD: −242.71; low evidence)
No increase in miscarriage risk. The miscarriage rate did not significantly differ between women who took antioxidants and those who did not. If anything, there was a slight trend toward fewer miscarriages in the supplement group, though this did not reach statistical significance. The important takeaway: there is no signal in this data that antioxidants make miscarriage more likely. (OR: 0.80; low evidence)
CoQ10 is not the same as "antioxidants"
The subgroup analysis by antioxidant type is where this paper gets genuinely useful.
CoQ10 was the only antioxidant that showed statistically significant improvements in clinical pregnancy rate when compared against placebo or no treatment (OR: 2.22; 95% CI: 1.57–3.14; p<0.00001; I²=0%). Melatonin, myo-inositol, vitamins, and combined antioxidants all showed numerical trends in the same direction, but none reached statistical significance.
CoQ10 also significantly increased the number of retrieved eggs and improved ovarian sensitivity (reduced gonadotropin dose). Melatonin showed significant improvements in embryo quality in some subgroups, but its effect on pregnancy rates was not statistically proven.
The practical implication: if you are taking a broad-spectrum antioxidant stack, the evidence base is largely built on CoQ10. The other compounds in the mix may contribute, but the data to prove it isn't there yet.
The Dose Paradox: More CoQ10 Is Not Better
Across antioxidant types, the analysis found a dose-dependent relationship that runs counter to most supplement marketing: lower doses produced better outcomes than higher ones.
For CoQ10 specifically, the subgroup data is striking:
30 mg/day: OR 2.76 (95% CI: 1.78–4.28; p<0.00001; I²=0%): statistically significant and highly consistent
600 mg/day: OR 1.62 (95% CI: 0.86–3.05; p=0.13): not statistically significant
1200 mg/day: OR 1.24 (95% CI: 0.34–4.45; p=0.75): not statistically significant
The 30mg dose outperformed doses 20 to 40 times higher. The researchers don't offer a definitive explanation, but the pattern held across multiple outcomes.
For melatonin, doses under 5 mg/day outperformed higher doses for embryo quality. The same "less is more" pattern appeared.
This matters because most CoQ10 supplements sold for fertility support are dosed at 200–600 mg/day. The strongest evidence in this paper is for a dose that most commercial products don't offer.
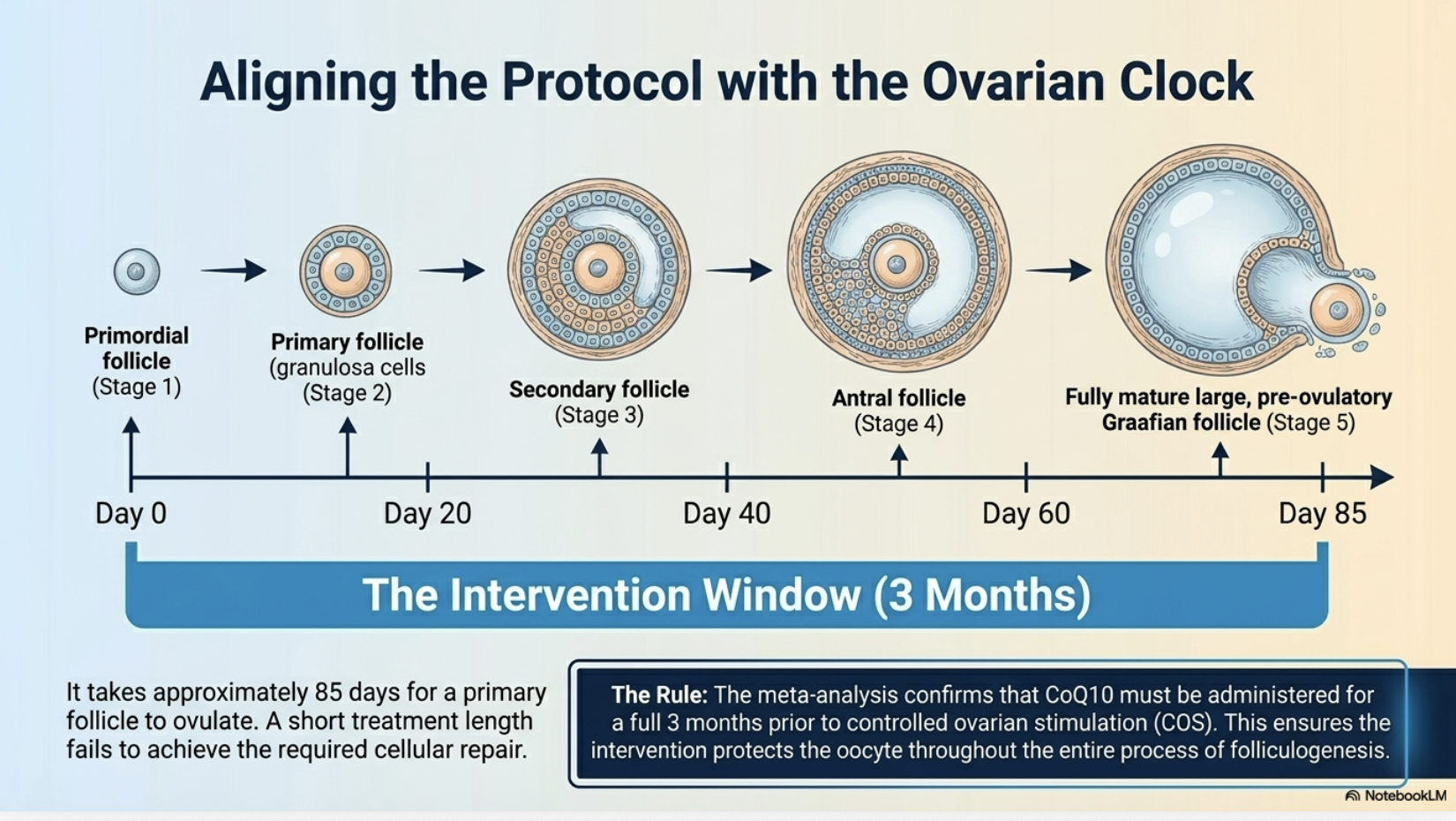
Timing Matters: Why Three Months Before Stimulation Is the Evidence-Based Window
When you start taking CoQ10 is just as important as the dose.
Starting CoQ10 three months before your stimulation cycle significantly improved clinical pregnancy rates. Starting two months before did not reach statistical significance. One month made no meaningful difference.
The reason comes down to biology. It takes roughly 85 days for a follicle to develop from its earliest stage to the point of ovulation. A three-month window means the CoQ10 is present throughout that entire process, supporting the egg from the beginning of its development rather than partway through. A shorter course likely does not give the supplement enough time to do anything useful.
Who benefits most from CoQ10
The timing and population subgroup data matters as much as the dose.
Duration: Starting CoQ10 three months before ovarian stimulation significantly improved clinical pregnancy rates (OR: 2.54; p<0.0001; I²=0%). Starting two months before did not reach statistical significance. The biology makes sense: follicle development takes approximately 85 days, so a three-month window covers the full maturation process.
Who it helps:
Women under 35 with diminished ovarian reserve: OR 2.38 (95% CI: 1.26–4.50; p=0.007): significant benefit
Women over 35 with diminished ovarian reserve: OR 2.07 (95% CI: 1.17–3.65; p=0.01): significant benefit
Women over 35 with suboptimal ovarian response (poor stimulation history but not classified as DOR): OR 1.38 (95% CI: 0.29–6.58; p=0.68): not statistically significant
The distinction between diminished ovarian reserve and suboptimal ovarian response is clinically relevant. CoQ10 showed consistent benefit for women with low reserve across age groups. For women whose reserve is relatively intact but who respond poorly to stimulation, the evidence is weaker.
What This Research Means for Women Considering Antioxidants
CoQ10 at 30 mg/day, started three months before stimulation, is the best-supported specific protocol in this data. This is considerably lower than most commercial fertility CoQ10 supplements. If you are using CoQ10 ahead of an IVF cycle, this regimen (not higher doses) is what the evidence points to.
The benefit appears most consistent for women with diminished ovarian reserve. Both under-35 and over-35 women with DOR showed significant improvements in clinical pregnancy rates. If your issue is low reserve specifically, the data is more supportive than if your issue is poor stimulation response with normal reserve.
Clinical pregnancy rate and live birth rate are different outcomes. Antioxidants showed a statistically significant effect on getting pregnant. They did not show a statistically proven effect on having a baby. This gap may simply reflect that not enough studies measured live birth, or it may reflect real limits to what antioxidants can achieve. More trials are needed before anyone can say which.
Miscarriage risk does not appear to increase. The trend in the data slightly favors fewer miscarriages in the antioxidant group, though this was not statistically significant. There is no signal here that antioxidants are harmful to pregnancy outcomes.
Antioxidants are a complementary strategy, not a primary treatment. The paper consistently frames these findings this way, and that framing is accurate. These supplements work within existing treatment protocols. They do not replace them, and they do not overcome the biological ceiling of significant ovarian aging.
What the Research Still Needs
Large-scale RCTs with live birth rate as the primary outcome, not egg counts or clinical pregnancy as proxies
Studies specifically designed to test whether the 30 mg/day CoQ10 finding holds in trials built around that dose
Trials in women without diminished ovarian reserve, to clarify who actually benefits
Longer follow-up on neonatal outcomes and birth defects; current safety data comes from trials too small to detect rare events
Standardized protocols across studies so dose, duration, and patient characteristics are directly comparable
Investigation into whether oral antioxidants and antioxidants added directly to the embryo culture medium work through different mechanisms
Common Questions About CoQ10, Melatonin, and Fertility Supplements
Q: Should I take CoQ10 before IVF if I have low ovarian reserve?
The evidence in this meta-analysis is the most supportive for women with diminished ovarian reserve, in both younger (under 35) and older age groups. The best-supported protocol is 30 mg/day started three months before your stimulation cycle. That said, this is a complementary strategy. It works alongside your treatment protocol, not instead of it. Discuss any supplementation with your reproductive endocrinologist before starting, particularly at non-standard doses.
Q: Why does 30 mg CoQ10 appear to work better than 600 mg?
The study found a consistent "less is more" pattern across antioxidant types, and the researchers note it across their findings. One possibility is that supraphysiological doses disrupt rather than support cellular antioxidant balance. However, the paper does not establish a confirmed mechanism — this is an observed pattern that needs direct investigation before it can be fully explained.
Q: Does taking antioxidants increase your chances of a live birth?
The honest answer is: the data doesn't prove it yet. Clinical pregnancy rates improved significantly. Live birth rates showed a non-significant odds ratio of 1.05 — meaning no detectable difference from placebo in the seven trials that measured this outcome. This may be because those trials were too small to detect a real effect, or it may mean the benefit doesn't extend all the way to delivery. More and larger trials are needed.
Q: Is melatonin worth taking for IVF?
Melatonin showed improvements in embryo quality in some subgroups, particularly at lower doses (under 5 mg/day). However, its effect on clinical pregnancy rates did not reach statistical significance. If embryo quality specifically is the concern, it may be worth discussing with your doctor. It did not show the same consistent pregnancy rate benefit as CoQ10.
Q: Are antioxidant supplements safe during fertility treatment?
Across five trials that reported adverse events, there was no statistically significant association between antioxidants and harm. However, those trials were not designed or powered to detect rare adverse events, and neonatal safety data is limited. "No significant association with adverse events" in a small trial is not the same as a comprehensive safety clearance. Discuss with your doctor before adding any supplement to an IVF protocol.
Source: Shang Y, Song N, He R, Wu M. Antioxidants and Fertility in Women with Ovarian Aging: A Systematic Review and Meta-Analysis. Adv Nutr. 2024;15(8):100273.
Read the full review article here → https://doi.org/10.1016/j.advnut.2024.100273