Minerals and Female Fertility: What 39 Studies Reveal About Selenium, Zinc, Iron, and More
Publication 17
What Your Body Does With Minerals Goes Far Beyond Bone Health
Most conversations about minerals and women's health stop at calcium and iron. But a 2024 systematic review published in Nutrients makes a broader case: the minerals in your body and the toxic metals you're exposed to have a measurable impact on whether eggs mature properly, whether embryos develop, and whether a pregnancy continues.
The same review that highlights selenium's importance also explicitly warns against supplementing without confirmed deficiency. The research is more nuanced than most fertility supplement marketing would have you believe, and that nuance is worth understanding.
Why This Systematic Review Is Worth Reading
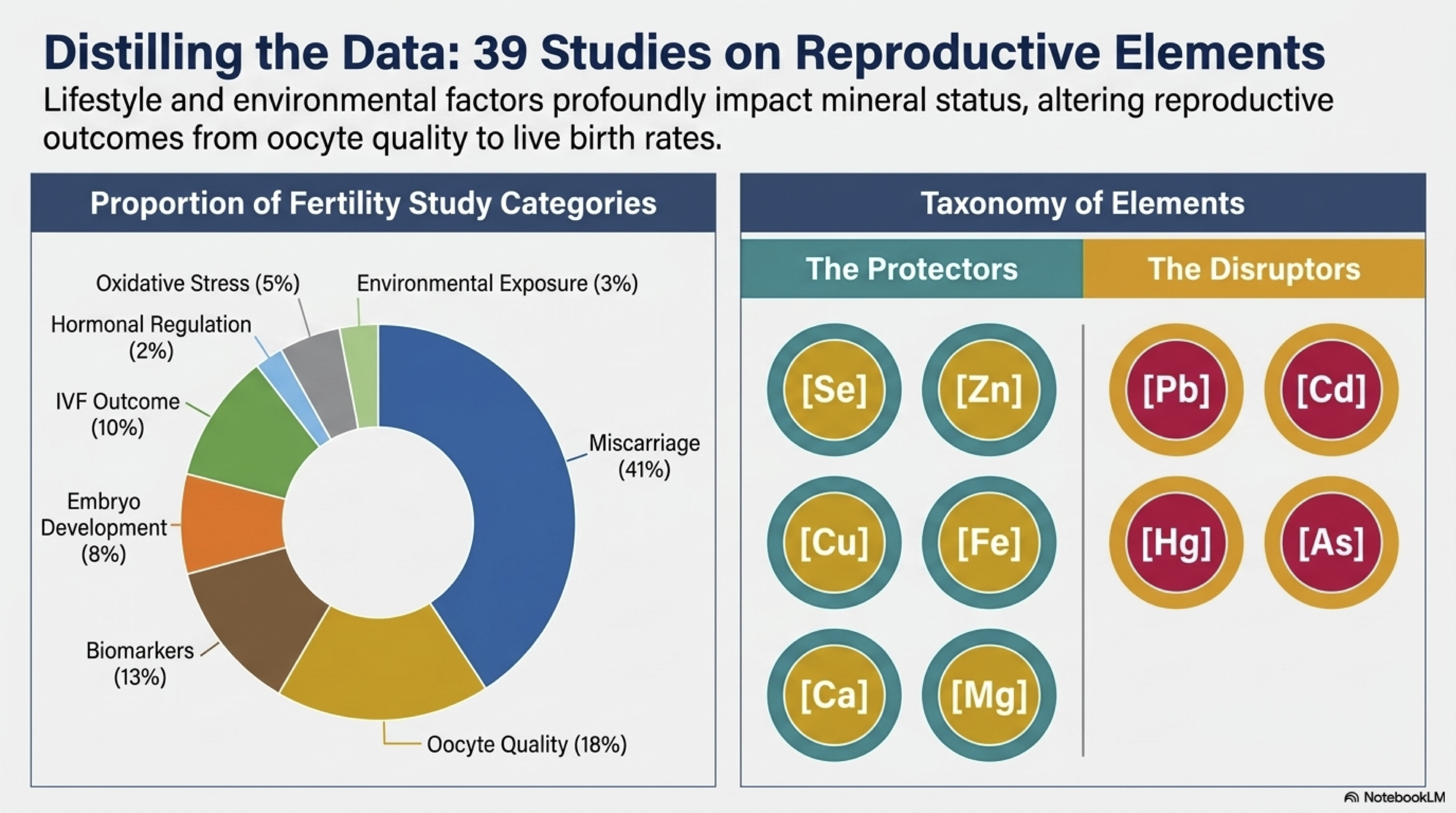
Study type: Systematic review (not a meta-analysis — findings are qualitative, not pooled statistics) Published: Nutrients, November 2024 (Kapper et al., Johannes Kepler University Linz) Scope: 39 studies selected from an initial pool of 20,830 records, covering minerals across eight reproductive outcomes.
The researchers included randomized controlled trials, prospective cohort studies, case-control studies, and observational studies, covering women planning pregnancy naturally and those using assisted reproduction technologies including IVF. Studies were assessed for quality using two validated tools: the Newcastle-Ottawa Scale for non-randomized studies and the Cochrane Risk of Bias tool for RCTs.
Of the 39 studies, 7 were high quality, 29 medium quality, and 3 low quality. That breakdown matters: the majority of findings are directional signals from medium-quality studies, not definitive proof. This review maps what the evidence currently points toward, not what has been conclusively established.
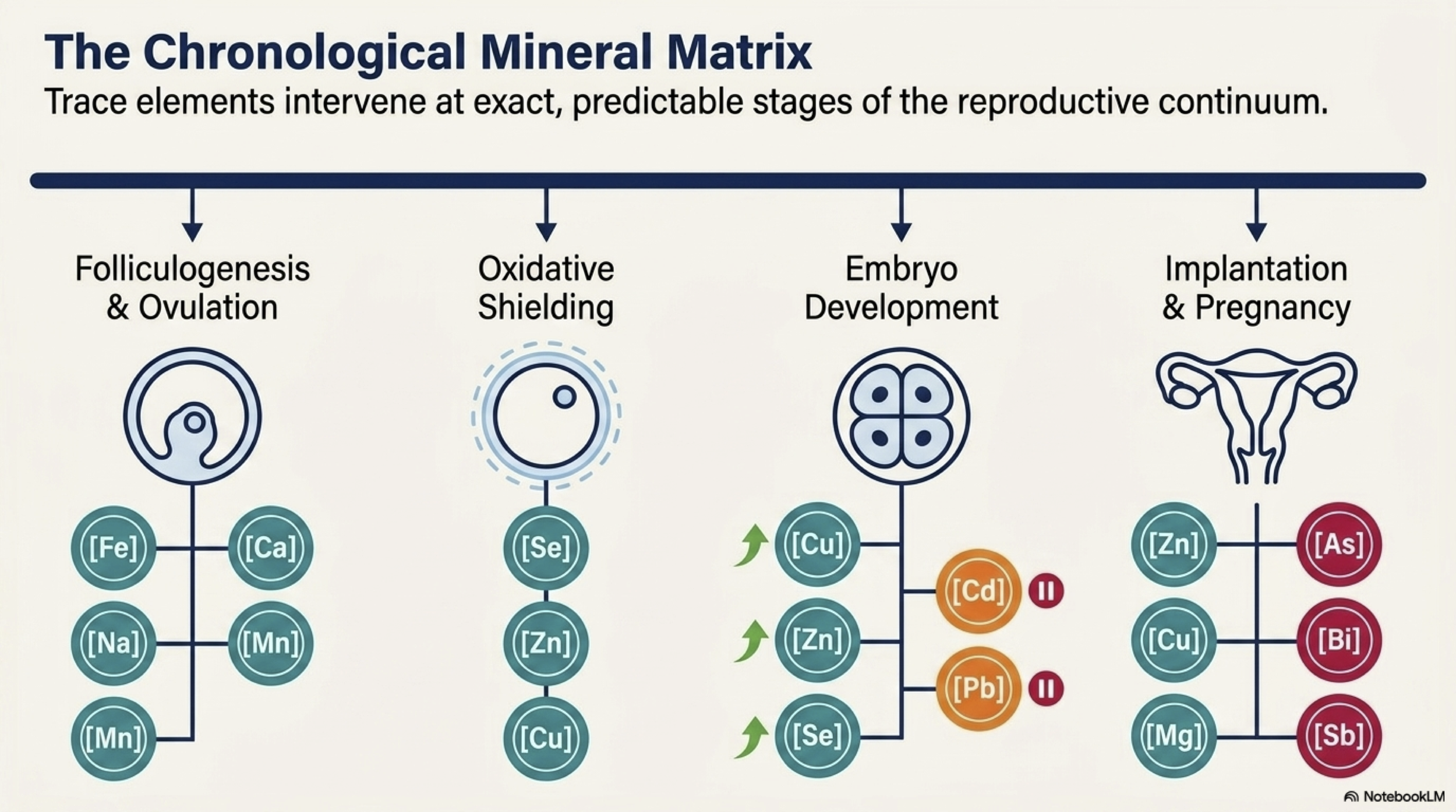
The eight reproductive areas covered: oocyte (egg) quality and ovulation, embryo development, oxidative stress, miscarriage, hormonal regulation, IVF outcomes, environmental mineral exposure, and minerals as biomarkers.
The Minerals That Consistently Support Fertility
Selenium: The Most Consistent Finding Across the Entire Review
Selenium appeared across more categories and more studies than any other mineral — and its absence was consistently associated with worse outcomes.
Egg and embryo quality. Women with endometriosis undergoing IVF had lower selenium levels in their follicular fluid (the fluid surrounding the egg) and higher markers of oxidative stress than women with other fertility diagnoses. Lower selenium was directly linked to poorer egg and embryo quality in that group.
Early embryo development. In women undergoing IVF, significantly lower selenium levels were found in the group whose embryos stopped developing in the earliest stages after fertilisation (a condition called early embryonic arrest). Women with higher selenium levels had better early development outcomes.
Miscarriage. This is where the selenium data is most consistent. Multiple studies found that women who miscarried had significantly lower selenium levels than those who did not. One study found women who miscarried averaged 66.71 ng/mL of selenium compared to 76.36 ng/mL in women with normal pregnancies. A pilot study found similarly lower red blood cell selenium in women with three or more unexplained pregnancy losses.
Preterm birth. A prospective cohort study of 1,197 women found that those in the lowest quartile of selenium at 12 weeks gestation had twice the risk of preterm birth compared to those with higher levels.
Environmental protection. Selenium also appears to offer a degree of protection against mercury exposure. Women with infertility had lower blood selenium levels and lower selenium-to-mercury ratios than fertile controls, suggesting selenium may partially buffer mercury's harmful effects on the reproductive system.
Zinc: Important at Every Stage
Zinc showed up consistently across egg quality, embryo development, miscarriage, and IVF outcomes.
Egg quality. Higher zinc in follicular fluid was associated with better oocyte yield and positively correlated with follicle number. In women with endometriosis undergoing IVF, higher intrafollicular zinc was associated with successful conception after treatment.
Embryo development. Higher zinc in follicular fluid was linked to faster embryo development. Low zinc was associated with early embryonic arrest.
Miscarriage. Multiple studies found lower zinc levels in women who miscarried compared to those who carried to term. Higher serum zinc after embryo transfer was associated with lower miscarriage risk in IVF.
IVF failure. A prospective cohort study of 305 women in China found that lower serum zinc increased the risk of IVF-embryo transfer failure by 66% in one of the two regional populations studied. The regional variation (Shandong vs. Beijing) was attributed to dietary differences, suggesting that local food environments and zinc intake matter.
Recommended daily intake: 8-11 mg. Optimal serum level: 80-120 µg/dL.
Copper: Beneficial in Balance, Harmful in Excess
Copper's picture is more complicated than selenium or zinc.
Higher copper levels in follicular fluid were associated with faster embryo development. Copper in the blood was elevated in pregnant women compared to non-pregnant women, and lower copper was found in women who miscarried and in those with primary infertility. One study found that higher blood copper during early pregnancy was associated with reduced miscarriage risk.
However, the review also notes that excess copper is associated with liver damage and oxidative stress. And in one study, follicular fluid copper at certain concentrations was not clearly beneficial for all outcomes. Copper is a mineral where the right range matters more than simply having more of it.
Iron: A Mineral Where More Is Not Always Better
Iron is perhaps the most instructive mineral in this review, because the evidence points in two directions depending on dose and context.
The case for iron. A large prospective cohort study following 18,555 premenopausal women over eight years found that women who took iron supplements had a 40% lower risk of developing ovulatory infertility compared to those who did not. A separate case-control study in Austria found that women with unexplained infertility frequently had ferritin levels below 30 µg/L, suggesting iron deficiency as a potential contributor to otherwise unexplained fertility problems. Iron also positively correlated with the number and maturity of eggs in follicular fluid.
The case for caution. An observational study of 582 women seeking fertility treatment found that iron supplementation above 45 mg/day was associated with decreased ovarian reserve, specifically fewer antral follicles and higher FSH levels. This suggests a potential toxic effect of excessive iron on ovarian function — a finding the authors flag as raising questions about gonadotoxicity at high doses.
The practical tension. Iron deficiency is common, particularly in reproductive-age women, and the data supports its importance for ovulation and egg quality. But exceeding the recommended dose appears to work against fertility rather than for it. This is a mineral where testing your actual levels before supplementing makes more sense than assuming more is better.
The Minerals That Harm Fertility
Not all minerals in this review are the kind you'd find in a supplement aisle. Lead, cadmium, and mercury appeared repeatedly as factors that worsen reproductive outcomes.
Lead and Spontaneous Abortion
A case-control study at Peking Union Medical College found significantly higher lead levels in women who had spontaneous abortions in the first 12 weeks (mean 27.17 µg/L) compared to women with viable pregnancies (mean 17.28 µg/L). The risk of miscarriage increased as lead levels rose, with levels above 10 µg/L particularly associated with early pregnancy loss.
A separate study also linked elevated lead to increased spontaneous abortion risk, though another found no significant association at very low blood lead levels (below 5 µg/dL) — suggesting that the threshold at which lead becomes harmful to early pregnancy may lie somewhere between these ranges.
Lead exposure comes primarily from old paint, contaminated water pipes, soil in urban areas, and certain occupational environments. It accumulates in the body over time.
Cadmium and Chromium as Biomarkers for Risk
A study tracking 195 pregnant women found that blood cadmium above 0.4 µg/L and urine chromium above 2 µg/L were significantly associated with higher odds of spontaneous abortion. The researchers proposed these as potential biomarkers for embryotoxicity risk.
Cadmium exposure comes primarily from cigarette smoke, contaminated food (particularly leafy vegetables, grains, and shellfish grown in contaminated soil), and some industrial environments. One study found that smoking significantly raised cadmium levels in women who miscarried, reinforcing smoking as a fertility risk through this specific pathway.
Mercury and Selenium's Protective Role
Women with infertility had lower blood selenium and lower selenium-to-mercury ratios than fertile controls, even after adjusting for age. The researchers suggest that selenium may offer partial protection against mercury's reproductive harm, and that a low selenium-to-mercury ratio may be a meaningful marker of fertility risk in women with environmental exposure.
Minerals and Miscarriage: The Most Studied Area
Miscarriage was the largest category in this review, with 16 studies examining the relationship. The most consistent pattern across them:
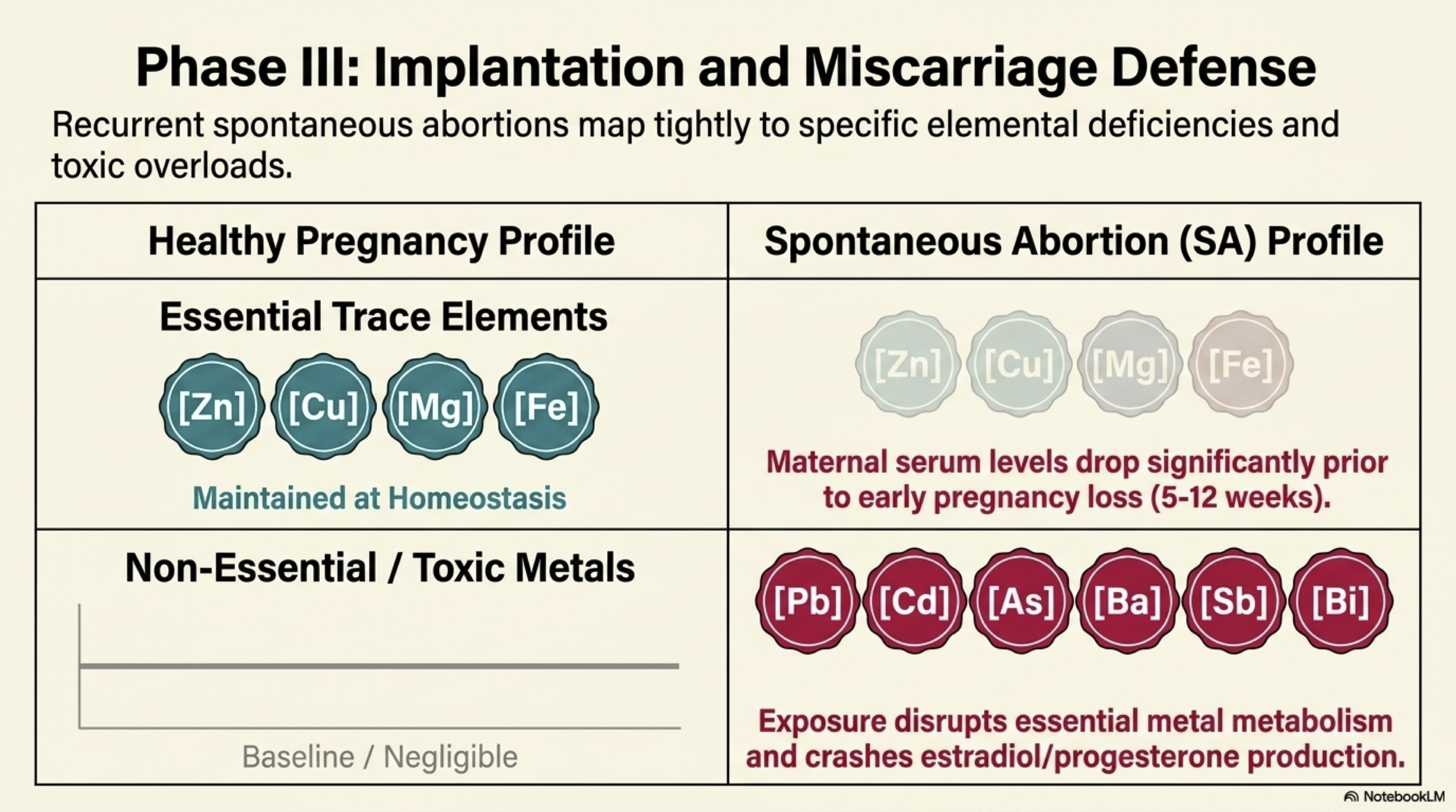
Protective: Higher levels of selenium, zinc, and copper were consistently associated with lower miscarriage risk across multiple independent studies in different populations.
Harmful: Higher levels of lead, arsenic, antimony, and cadmium were associated with increased miscarriage risk. Non-essential metals (those with no biological role in the body) in particular showed associations with disrupted hormone levels and early pregnancy loss. One study found that spontaneous abortions in the first trimester were associated with higher arsenic, antimony, and bismuth alongside lower estradiol and progesterone.
Nuanced: Not all studies agreed, particularly around lead at low levels. And one study that compared women at very different reproductive stages (miscarriage, postpartum, pregnant) may have introduced metabolic differences that confounded the mineral measurements — the review notes this limitation explicitly.
The overall picture is directional: adequate essential mineral status and low toxic metal exposure both appear relevant to miscarriage risk. But this is observational data across diverse populations, not proof of direct cause and effect.
Minerals and IVF: What the Data Shows
Four studies looked specifically at mineral levels and IVF outcomes.
Zinc and IVF failure. Low serum zinc increased IVF failure rates significantly in one regional Chinese population, with the 66% increased risk figure mentioned above. The researchers suggested that dietary zinc intake — which varies considerably by region and diet — may be a modifiable factor for women preparing for IVF.
The calcium-to-magnesium ratio. A multicenter randomized prospective study found that a higher calcium-to-magnesium ratio before ovarian stimulation was associated with significantly better odds of biochemical pregnancy, clinical pregnancy, and live birth. Women with a Ca/Mg ratio of 5.02 or above had meaningfully better outcomes than those with a lower ratio. This is a less-discussed angle — most IVF nutrition conversations focus on individual minerals, not their ratios.
Mineral levels in IVF women vs. controls. A controlled trial found that women undergoing IVF had lower selenium, zinc, and copper in their serum and follicular fluid compared to women not undergoing IVF. Multivitamin/mineral supplementation for 45 days normalized these levels, creating what the researchers described as a more favorable biochemical environment for egg development. This does not prove that supplementation improved outcomes, but it does suggest that the IVF process itself may affect mineral balance.
Toxic minerals and IVF. Higher follicular fluid chromium and manganese were associated with lower mature egg proportion, while follicular fluid zinc was inversely related to fertilization rates at certain concentrations — illustrating that even beneficial minerals can have complex concentration-dependent effects in the follicular environment specifically.
Minerals, Hormones, and Ovulation
Only one study directly examined the relationship between dietary mineral intake and hormone levels in healthy women. This is a gap the review explicitly flags as a limitation of the current literature.
That study, conducted in 259 healthy, regularly menstruating women, found that low sodium intake (below 1,500 mg/day) was associated with increased FSH and LH and decreased progesterone, along with an elevated risk of anovulation (cycles where no egg is released). Low manganese intake was also linked to increased anovulation risk.
This is a single prospective cohort study, so the findings should be treated as preliminary. But the suggestion that sodium, a mineral not typically associated with reproductive health, may influence ovulatory hormones when intake is very low is worth noting.
The Most Important Caveat in This Entire Review
The researchers state this directly: supplementation should only be considered when a deficiency has been identified through testing. Without a confirmed deficiency or medical indication, mineral supplementation could cause more harm than benefit.
This caveat is not boilerplate disclaimer language. It reflects findings within the review itself. Excess iron was linked to reduced ovarian reserve. Excess copper is associated with liver damage. Excess calcium and sodium were associated with lower egg quality. The dose-response relationship for minerals is not linear and more is not always better, and in some cases it is clearly worse.
This is relevant because fertility supplements often contain multiple minerals at doses that assume deficiency. For someone with adequate levels, adding high-dose selenium or copper doesn't produce the benefits seen in deficient populations and may introduce risk. The research supports testing first, then supplementing with clinical guidance if deficiency is confirmed.
Limitations and Gaps in This Research
The majority of studies (74%) are medium quality, primarily case-control or observational designs. These can identify associations but cannot prove that mineral levels caused the outcomes observed.
Most studies measured mineral levels at a single point in time, which doesn't capture how levels fluctuate across the menstrual cycle or during early pregnancy.
No standardized supplementation protocols exist across the included studies, making it difficult to draw conclusions about specific doses.
Geographic and dietary variation between populations limits how broadly findings can be applied.
Despite ovulation being central to fertility, only one study in this review examined how minerals affect the hormones that control it. If your concern is irregular cycles or whether you are ovulating at all, this review has almost nothing to say about that.
Sample sizes varied widely, with some studies involving fewer than 30 participants.
The review includes studies across multiple continents and populations, but did not analyze whether findings differed significantly by geography, diet, or baseline mineral status.
What This Research Means for Women Thinking About Fertility
Selenium, zinc, and copper are the minerals with the most consistent evidence for supporting fertility. Deficiencies in all three have been linked to poorer egg quality, higher miscarriage risk, and worse embryo development across multiple independent studies. If you are preparing for pregnancy or undergoing IVF, having these levels tested is a reasonable step.
Iron requires balance, not maximizing. The evidence supports iron's role in ovulation and egg maturity, but excessive supplementation (above 45 mg/day) may reduce ovarian reserve. If you are supplementing iron, know your ferritin level first.
Toxic metal exposure is a real and underappreciated factor. Lead, cadmium, and mercury showed consistent associations with miscarriage and fertility disruption. Reducing exposure where possible — avoiding smoking, filtering drinking water if you live in an older building, being aware of cadmium-contaminated food sources — is a practical step with evidence behind it.
The calcium-to-magnesium ratio may matter for IVF. This is less well-established but worth discussing with your reproductive endocrinologist if you are preparing for an IVF cycle.
Test before you supplement. This review's own conclusion is that mineral supplementation without confirmed deficiency may cause more harm than benefit. A serum mineral panel is a more useful starting point than a broad-spectrum fertility supplement.
Source: Kapper C, Stelzl P, Oppelt P, et al. The Impact of Minerals on Female Fertility: A Systematic Review. Nutrients. 2024;16(23):4068. Published 2024 Nov 27. doi:10.3390/nu16234068
Read the full text here → https://www.mdpi.com/2072-6643/16/23/4068